
“Every physiological strain applied to the patient will induce extra stress on top of stress related to the disease or injury of the patient.”[1]
The electric thermostat was invented in 1883 by Warren Johnson, a Professor of Natural Science at the State Normal School in Whitewater (destined to become the University of Wisconsin–Whitewater in 1971), who had grown weary of temperature extremes in his classroom. So he went to work, and patented his invention as the “electric tele-thermoscope” on July 24. It proved to be a break-through invention that “ brought order, automation and comfort to a previously chaotic system” and led to Johnson’s retirement from teaching and founding of his company, Johnson Controls.
But Johnson could not leave well enough alone. When it came to room temperature regulation, he wanted to make good matters better. So 12 years later, in 1895, he patented the successor to the electric thermostat: the pneumatic thermostat. It was the first automatic multi-room temperature control system intended for use in commercial buildings, hotels, schools – and hospitals.

Warren Johnson, whose invention of the electric thermostat in 1883 and pneumatic thermostat in 1895 ushered in the era of “smart” buildings with room temperature control.
By the turn of the century, things had cooled down and warmed up, temperature-wise. On July 27, 1903, Belfast’s Royal Victoria Hospital opened its doors and, lo and behold, temperature and humidity were effectively controlled in each and every room. What a marvel of modern science. The grand opening was presided over by no less than King Edward VII and Queen Mary, and the ceremony was followed by an explosion of civic pride. What a hospital! It was not only the state-of-the-art pavilion design that excited city residents, but the remarkably modern room ventilation system that controlled temperature in each and every room. The hospital was the first air-conditioned public building in the world.[2] This was no small achievement, and over a century later, in 2018, the hospital received a prestigious Engineering Heritage Award from the UK Institution of Mechanical Engineers.
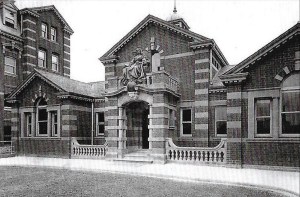
The Royal Victoria Hospital, Belfast, 1903. A statue of Queen Victoria sits above the main entrance.
At the grand opening, a newly commissioned statue of Queen Victoria was placed above the front entrance. This was in 1903. Why then, 123 years later, during my hospitalization for open-heart surgery, did Cooperman Barnabas Medical Center assign me a room without working temperature control? The nursing staff was unconcerned. “Yes,” remarked one nurse, “some of the rooms are too hot and some too cold, ” and let it go at that.
Huh? My room gave me the worst of both worlds. It ricocheted between extremes, leaving me too uncomfortable to the point of being unable to sleep. I suffer from peripheral neuropathy, and it was cruelly exacerbated by the night-time heat. So I complain. But four successive visits from engineering department personnel, laden with ladders and tools, do little if any good. After each engineering house call, I am assured that temperature control has been restored and the room will gradually become comfortable.
But it does not. I continued my stay in a room that was either an oven or a refrigerator. Perhaps it was a foretaste of hell. Where was Warren Johnson when I needed him? My discomfort heightens, and I was approaching wit’s end. Owing to the neuropathy, I couldn’t tolerate the heat in particular. Finally, after nights of mounting misery, I called my wife during the night and asked her to call the nurses’ station – it was not responsive to my pleas for temperature rescue – and speak with the nurse supervisor. She told them I was desperate and at the point of walking out of the hospital in the interest not of health, but of survival.
Her call does the trick. Several nurses loudly march into the room and announce they are moving me to another room. They do so and, lo and behold, the new room has the same defect as the previous one. I tolerate two more nights in a prison of hot and cold before I am discharged to the normal, post-Warren Johnson twenty-first-century world of room temperature control.
____________________
“Yes, some of the rooms are too hot and some too cold.” May I suggest that the nurse who responded thusly to my complaint of room temperature dysregulation could stand a little education. For one thing, it should be explained to her and her colleagues that thermal comfort of hospitalized patients can differ from that of healthy persons; this is because a physical disability, including post-operative status, affects thermophysiology, thermal sensation, metabolism, blood flow, and regulatory responses such as vasomotor control and body skin temperature and the ability to sweat.
It follows that temperature regulation in hospital rooms is not simply a matter of patient “comfort” and “well-being” in some vague, nondescript sense.[3] Studies have linked poor temperature control in hospital rooms to medical complications that affect recovery. Temperature regulation has been linked, inter alia, to prevention of bacterial and viral growth within the hospital.[4] A scoping review of 11 clinical trials and cross-sectional studies underscored the benefits of installing modern HVAC (heating, ventilation, air conditioning) systems in hospitals in terms of heat stress protection and support of thermoregulation.[5]
More specific to cardiac surgery is the risk of neurological injury associated with hyperthermia – an increase in core body temperature – and hyperthermia can indeed result from excessively warm hospital rooms.[6] What are the consequences? Even a slight rise in body temperature “aggravates ischemic neuronal injury and accelerates neuronal death.” Following from such neurological injury, postoperative hyperthermia correlates with heightened cognitive dysfunction, as measured six weeks after cardiac surgery.[7]
Perhaps the lack of thermal control I encountered in two hospital rooms has now been rectified. I hope so. But the memory of post-operative heat stress lingers. Let there be no doubt: Room 2408, the site of heat stress and sleeplessness beyond that resulting from open-heart surgery, is emblazoned in my psyche.
__________________
Immediately after relocating me, Room 2408 was cordoned off as unfit for patient (i.e., human) habitation and scheduled for a complete revamping of the room’s temperature control system. Was the additional work of the engineering crew successful? I hope so. But I urge readers not to find out. If you ever find yourself in Cooperman Barnabas Medical Center, stay away from Room 2408. Indeed, play it safe and keep out of Room 2408 in any and all hospitals. The medical care that awaits you may be exemplary, but you could still get burned.
______________________
[1] Jan Verheyen, “Thermal Comfort of Patients: Objective and Subjective Measurements in Patient Rooms of a Belgian Healthcare Facility,” Building and Environment, 46:1195-1204, 2011.
[2] Monica Monaghan & Alun Evans, “The Royal Victoria Hospital, Belfast” (www.ahajournals.org).
[3] Verheyen, op cit., pp. 1195-1196.
[4] TCRS, “Importance of Temperature Control in Healthcare Facilities” (https://www.tcrentalsolutions.com/blog/temperature-in-healthcare).
[5] Benedikt Lenzer, et al., “Health Effects of Heating, Ventilation and Air Conditioning on Hospital Patients: A Scoping Review,” BMC Public Health, 20:1287, 2020 (https://doi.org/10.1186/s12889-020-09358-1).
[6] Nancy A Nussmeier, “Management of Temperature During and After Cardiac Surgery,” Texas Heart Institute Journal, 32:472–476, 2005.
[7] Ibid., p. 474.
Copyright © 2026 by Paul E. Stepansky. All rights reserved. The author kindly requests that educators using his blog essays in their courses and seminars let him know via info[at]keynote-books.com.







